A gastrostomy tube (also called a g-tube) is a medical device used to feed newborns who can’t feed through normal methods. G-tubes can be temporary or permanent and are often considered for long term care.
The information in this post was compiled from government, educational non-profit, and medical expert sources.
To learn about G-tubes, including the placement procedure, care, and long term outlook, keep reading.
What Is a G-Tube (Gastrostomy Tube)?
A G-tube consists of several parts.
There is a feeding port that is inserted into the child’s abdominal wall. The feeding port connects the inside of the child’s stomach to the surface of the child’s belly through what is called a stoma.
On the outside, there is an extension tube. One side of the tube connects to the feeding port, and the side connects to the feeding syringe or feeding pump (which is then attached to a feeding bag).
Along the tube, there is often also a clamp. The clamp works as a valve to control the flow of nutrients.
Why Do Doctors Recommend a G-Tube for Infants?
Doctors may recommend a G-tube when a baby has serious medical issues that prevent the baby from being able to feed normally (either by breastfeeding or bottle feeding).
If other less invasive or temporary treatment strategies can be used effectively to solve the baby’s feeding problems, then a G-tube may not be necessary. Although a G-tube can be used temporarily and then removed, it is often considered for more long term treatment strategies.
An infant discharged from the NICU with a G-tube can be fed by parents at home. However, parents should always be educated about how to properly use, clean, and maintain a G-tube before taking the child home.
How Are G-Tubes Placed?
G-tubes are placed in one of three ways: either by laparoscopic surgery, by open surgery, or by percutaneous endoscopic gastrostomy (commonly called the PEG procedure).
Laparoscopic surgery: two small cuts are made in the belly and the G-tube is guided in using a laparoscope, which is a tiny telescope.
Open surgery: similar to laparoscopic surgery, except larger incisions are made and the telescope is not used.
The PEG procedure: an endoscope (a tiny camera on a tube) is inserted through the mouth, down the esophagus, and into the stomach, where the surgeon uses the camera feed to guide the G-tube placement.
The procedure usually takes under an hour to complete.
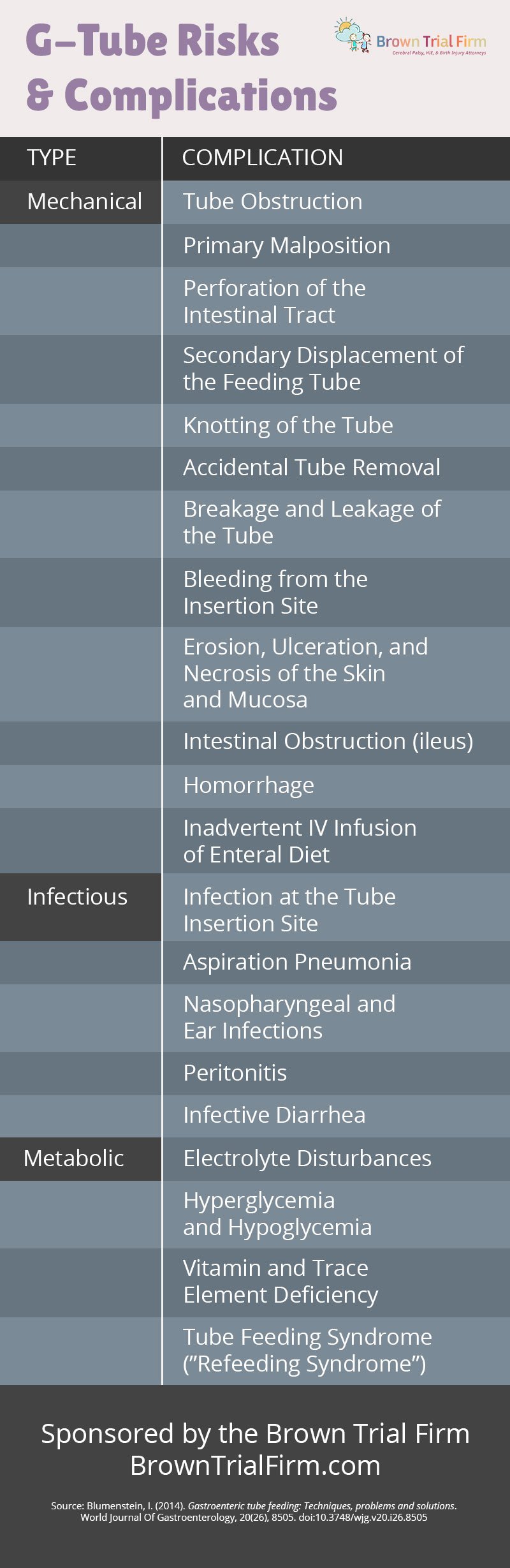
G-Tube Risks & Complications
The success rate of the placement procedure has been measured at upwards of 86-97% depending primarily on the experience of the surgeon. After a successful placement, there are a number of potential complications to be aware of.
- Tube Obstruction
- Primary Malposition
- Perforation of the Intestinal Tract
- Secondary Displacement of the Feeding Tube
- Knotting of the Tube
- Accidental Tube Removal
- Breakage and Leakage of the Tube
- Bleeding from the Insertion Site
- Erosion, Ulceration and Necrosis of the Skin and Mucosa
- Intestinal Obstruction (ileus)
- Hemorrhage
- Inadvertent IV Infusion of Enteral Diet
- Infection at the Tube Insertion Site
- Aspiration Pneumonia
- Nasopharyngeal and Ear Infections
- Peritonitis
- Infective Diarrhea
- Electrolyte Disturbances
- Hyperglycemia and Hypoglycemia
- Vitamin and Trace Element Deficiency
- Tube Feeding Syndrome (“Refeeding Syndrome”)
We have made an infographic containing those potential risks:
Additional Questions About G-Tubes?
If your baby was sent home from the NICU with a G-tube and you have questions about why, or other related conditions, such as birth asphyxia, Hypoxic-Ischemic Encephalopathy (HIE), Cerebral Palsy, or other birth injuries, please contact us today. We can help find answers to your questions and determine whether a preventable medical error occurred.
Sources:
Blumenstein, I. (2014). Gastroenteric tube feeding: Techniques, problems and solutions. World Journal Of Gastroenterology, 20(26), 8505. doi:10.3748/wjg.v20.i26.8505
How Gastrostomy Tubes Help Preemies With Nutrition. (2020). Verywell Family. Retrieved 3 March 2020, from https://www.verywellfamily.com/gastrostomy-tubes-in-preemies-2748649
Contact a Cerebral Palsy and Birth Injury Attorney
Getting help for a child with a birth injury can make a big difference. Early intervention and early treatment is often key to helping improve a child’s wellbeing. You must act quickly.
If you have questions about whether your child’s birth injury was caused by a preventable medical error, then our attorneys at Brown Trial Firm may be able to help.
Case Review at No Cost or Obligation
If you would like help investigating your child’s birth injury, please contact us. Our birth injury attorneys will be happy to give you a free case evaluation. We can also point you to great non-legal resources that can help you figure out your next steps.
Many birth injuries that cause cerebral palsy could have been prevented. Don’t wait, get help today. Call +1 (866) 393-2611, email us at [email protected], or use the live chat button for 24/7 assistance.
- Cerebral Palsy
- Caput Succedaneum and Cephalohematoma
- Neonatal Intracranial Hemorrhage (Childbirth Brain Bleeds)
- Hydrocephalus (Extra Fluid in the Brain Cavity)
- Cervical Dystonia
- Hemiplegia (Brain or Spinal Cord Injury)
- Hemorrhagic Stroke
- Neonatal Stroke
- HIE
- Periventricular Leukomalacia (PVL) Brain Injury
- Infant Seizures
- Spastic Diplegia (Spasticity in the Legs)
- Top Risks for Birth Injuries
- Fetal Alcohol Syndrome
- Facial Paralysis
- Spinal Cord Injuries
- Bell’s Palsy
- Brachial Plexus Nerves & Erb’s Palsy
- Klumpke’s Palsy
- G-Tubes for Newborns
- Medical Errors
- Cesarean Section & Birth Injury
- Negligence in Brain Cooling Treatment
- Craniosacral Therapy
- Occupational Therapy
- Speech Therapy
- Transition From Pediatric to Adult Healthcare
- Surgical Options for Spastic Cerebral Palsy
- Fetal Intolerance to Labor
- Jaundice (Kernicterus)
- Breech Position
- Placental Complications
- Umbilical Cord Problems
- Uterine Rupture
- Cervical Incompetence (Insufficiency)
- Blighted Ovum
- Necrotizing Enterocolitis (NEC) - Intestinal Inflammation
- Cephalopelvic Disproportion
- Meconium Aspiration Syndrome
- Amniotic Fluid Embolism
- Birth Injury from Premature Delivery
- Developmental Delays
- Abnormal Cord Insertion
- Infections at Birth
- Chorioamnionitis Bacterial Infection
- Premature birth
- Oxygen Deprivation
- Listeria
- Birth-Acquired Herpes
- Placenta Previa
- Placental Abruption
- Mismanaged Fetal Malposition
- Rapid Labor
- Obesity Related Birth Injuries
- Intrauterine Growth Restriction
- Blood Clots During Pregnancy
- Ectopic Pregnancy Misdiagnosis
- Myths & Facts About Birth Injuries
- Bacterial Vaginosis
- Gestational Diabetes
- Maternal Mortality Risk
- Oligohydramnios (Low Amniotic Fluid)
- Infections During Pregnancy
- Excessive Bleeding During Pregnancy
- Congenital Syphilis


