An umbilical cord may become compressed or damaged before or during childbirth. Common signs of umbilical cord problems include an irregular fetal heartbeat and decreased fetal movement. Umbilical cord problems can be a serious threat to a fetus’s health and should be carefully monitored and treated as necessary.
The information in this post was compiled from government, educational non-profit and medical expert sources.
Keep reading to learn about the signs of umbilical cord problems.
What does the umbilical cord do?
Before exploring the common problems with umbilical cords, we should first examine why the umbilical cord is so important.
The umbilical cord connects the mother to the baby as the baby develops in the womb. The umbilical cord starts at the mother’s placenta and connects to an opening in the baby’s stomach.
During pregnancy, the umbilical cord delivers vital nutrients and oxygen from the mother to the baby. The umbilical cord has 1 vein and 2 arteries surrounded by a protective layer. The protective layer is made up of a substance called Wharton’s jelly and is wrapped in a membrane called the amnion.
The vein delivers blood full of nutrients and oxygen to the baby, while the arteries remove deoxygenated blood and waste from the baby back to the placenta.
After the baby is born, the umbilical cord is clamped and cut. There are no nerves within an umbilical cord, so this is not painful for the baby or the mother. Within a couple of weeks, the clamped stump of the umbilical cord eventually falls off, leaving behind the baby’s belly button.
Most common umbilical cord problems
Below are some of the most common umbilical cord issues that can interfere with the health of a baby:
- Umbilical cord compression
- Nuchal cords
- True knots
- Umbilical cord prolapse
- Short umbilical cords
- Vasa previa
- Umbilical cord infection
In the next sections, we will discuss the signs of each problem and what each means for the health of the fetus.
Umbilical cord compression
One common umbilical cord problem is compression. Compression occurs for a number of reasons, but it ultimately leads to decreased blood flow through the umbilical cord. Babies can survive short periods of umbilical cord compression, but if an adequate flow of blood to the baby is not re-established, the baby may suffer serious birth injuries. As we covered in the previous sections, this condition is dangerous because babies need nutrients and oxygen to remain healthy during development.
Signs of umbilical cord compression may include less activity from the baby, observed as a decrease in movement, or an irregular heartbeat, which can be observed by fetal heart monitoring.
Common causes of umbilical cord compression include:
- Nuchal cords
- True knots
- Umbilical cord prolapse
Nuchal cords
Nuchal cord is the medical term for when an umbilical cord becomes wrapped 1 or more times around the baby’s neck within the womb. Nuchal cords are fairly common, occurring in approximately 20 to 30% of deliveries.
A nuchal cord is usually caused by the baby’s movement through a loop of the umbilical cord. Nuchal cords may be detectable by electronic fetal heart monitoring or ultrasound. Certain patterns of the baby’s heart rate, like “variable decelerations” of the heart rate, are often associated with nuchal cords.
A nuchal cord can become dangerous if the cord wraps tightly around the baby’s neck during labor and delivery, and the flow of blood to the baby is interrupted.
In a dangerous situation caused by a nuchal cord, a cesarean section (C-section) delivery may be necessary to quickly deliver the baby before the lack of blood flow causes the baby to suffer a permanent brain injury.
While complications of nuchal cords are rare and can typically be avoided with appropriate medical care, some long-term effects a baby can suffer include the following:
- Cerebral palsy. Cerebral palsy is a common complication of oxygen deprivation in newborns that sometimes occurs when the umbilical cord wraps around the child’s neck during delivery. It can affect a child’s cognitive and neurological abilities and may be mild or severe. Cerebral palsy is a permanent condition that requires care for the child’s lifetime.
- Epilepsy. Some babies develop epilepsy from having the umbilical cord around their necks during delivery. The condition causes seizures and can range from mild to severe.
- Hypoxic-ischemic encephalopathy (HIE). Lack of oxygen to the brain due to nuchal cord problems can lead to HIE, which often results in developmental disabilities or delays. Some of these can be cognitive and others physical.
- Stillbirth. In rare instances, problems with nuchal cords during delivery can lead to stillbirth.
True knots
True knots are the medical term for when the umbilical cord gets twisted like a rope into a knot. True knots can form simply by the baby’s movement within the mother’s womb. Other causes can include the following:
- Monoamniotic twins (when twins share the same amniotic sac)
- Polyhydramnios (excessive amounts of amniotic fluid)
- Overly long umbilical cords
- Smaller than normal fetuses
- Gestational diabetes
- Amniocentesis (a procedure to test the amniotic fluid)
True knots also form more often in male fetuses or when the mother has had several previous pregnancies.
If a baby’s activity decreases after 37 weeks, that is a common sign of a true knot. Medical professionals should remain alert for decreased activity and should test for umbilical cord problems as needed.
Medical professionals should monitor a baby’s heartbeat and activity to determine whether further intervention is required.
Umbilical cord prolapse
An umbilical cord prolapse means that the umbilical cord has moved down the birth canal before or alongside the baby. Ideally, the umbilical cord should follow the baby out through the birth canal. If the cord gets ahead of the baby or moves alongside the baby, a dangerous situation can develop, leading to birth asphyxia, HIE and other birth injuries.
If a mother or a medical professional becomes aware of a possible cord prolapse, the medical professionals should take immediate steps to monitor and intervene as necessary—particularly if the prolapse occurs in the third trimester. By carefully monitoring the situation and by delivering the baby by C-section, potentially serious injuries can be avoided.
Short umbilical cords
If the baby’s umbilical cord is short, the baby’s movements may stretch and tear either the umbilical cord or the mother’s placenta (known as placental abruption). Ideally, an umbilical cord should be long enough for the baby to move without stretching the cord but not so long as to easily get knotted or tangled.
If a short umbilical cord causes placental abruption, the mother may hemorrhage large amounts of blood, which can be harmful to both the baby and the mother. Medical professionals should be prepared to perform a C-section or a delivery with forceps or a vacuum extractor (although forceps and vacuum extractor methods can also be dangerous).
Vasa previa
Vasa (from the Latin for vessels) previa (from the Latin for before) is a rare condition where unprotected blood vessels of the umbilical cord are positioned over the cervix. In this position, the vessels are at risk for rupture during labor and delivery, which can lead to massive blood loss and permanent injury to the baby.
If vasa previa is detected, medical professionals should consider an early C-section to prevent potential birth injuries. If the blood vessels are ruptured during delivery, a blood transfusion may be necessary immediately after birth.
Umbilical cord infection
When the fetal membranes become infected, that infection can spread to the umbilical cord, the placenta, the fetus and the amniotic fluid. This is called an intra-amniotic infection or an IAI.
An IAI or an infection of the umbilical cord is called funisitis. An infection of the umbilical cord can potentially lead to fetal inflammatory response syndrome, or FIRS, and can cause the following:
- Preterm birth
- Neonatal sepsis
- Periventricular leukomalacia
- Cerebral palsy
Antibiotics can potentially prevent a serious birth injury from occurring.
Treatment for umbilical cord-based injuries
Careful monitoring, an early C-section or operative delivery, and blood transfusions are all potential treatment strategies to prevent injuries caused by umbilical cord problems.
An additional treatment strategy that is available once the child has been delivered is cooling therapy. Cooling therapy can be used shortly after birth to try to slow or stop permanent injuries caused by a lack of blood flow to the brain.
<a href="https://browntrialfirm.com/" target="blank"><img src="https://browntrialfirm.com/infographics/infant-cooling-therapy-btf.jpg" alt="Cooling Therapy Infographic" title="" style="width: 100%; max-width: 800px; display: block; margin: 15px auto;" /></a>
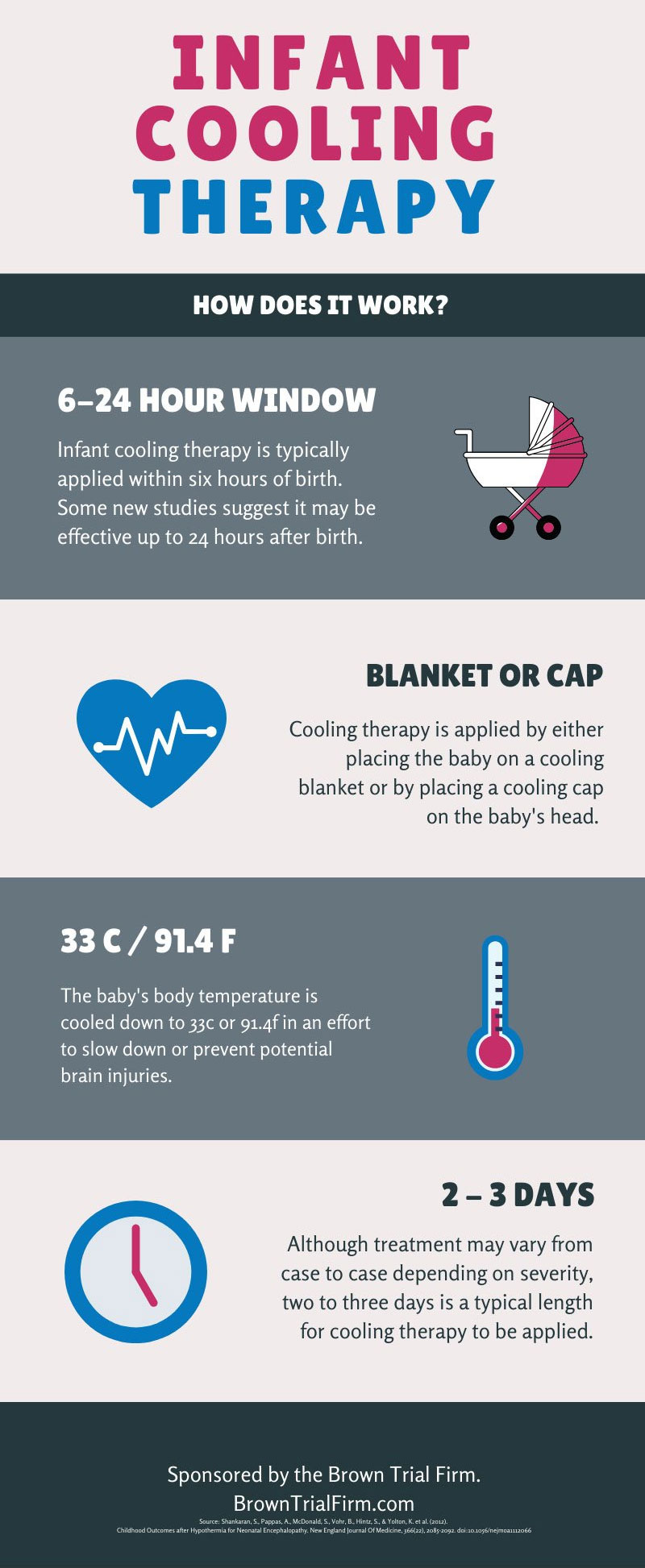
Infant cooling therapy basics
How soon does cooling therapy need to be started after birth?
Infant cooling therapy is typically applied within 6 hours of birth. Some new studies suggest it may be effective up to 24 hours after birth.
Cooling therapy is applied by either placing the baby on a cooling blanket or by placing a cooling cap on the baby’s head.
The baby’s body temperature is cooled down to 33 degrees Celsius or 91.4 degrees Fahrenheit in an effort to slow down or prevent potential brain injuries.
Although treatment may vary from case to case depending on severity, 2 to 3 days is a typical length for cooling therapy to be applied.
Sources:
What is the umbilical cord?. (2018). nhs.uk. Retrieved 17 February 2020, from https://www.nhs.uk/pregnancy/
Umbilical cord conditions. (2020). Marchofdimes.org. Retrieved 17 February 2020, from https://www.marchofdimes.org/find-support/topics/birth/umbilical-cord-conditions
What happens if the umbilical cord is around my baby’s neck? | Your Pregnancy Matters | UT Southwestern Medical Center. (2020). Utswmed.org. Retrieved 17 February 2020, from https://utswmed.org/medblog/nuchal-cord-during-pregnancy/
FAQs
When should I worry about fetal hiccups?
Many babies have hiccups while in the womb. Fetal hiccups occur when the baby takes in amniotic fluid as their lungs develop and are completely normal starting in the later portion of the first trimester and can even be viewed on an ultrasound.
Some limited studies on animals have linked problems with the umbilical cord when fetal hiccups occur later in pregnancy. Specifically, researchers involved in such studies believe it’s possible that hiccups might indicate compression or prolapse of the umbilical cord. However, these studies have only been done on animals, so it’s not certain that this is the case in humans.
Some mothers might be worried about fetal hiccups. Earlier in pregnancy, they shouldn’t be of any concern, but if a change suddenly occurs past the 28th week and they become stronger, it’s wise to consult with the doctor. A medical exam can help determine if there are any issues with the umbilical cord that need to be addressed.
How can a short umbilical cord be prevented?
Unfortunately, there are no definitive ways to prevent a short umbilical cord to minimize the risks associated with it, such as placental abruption. However, there are certain factors that may contribute to the development of a short umbilical cord, such as:
- Drinking alcohol during pregnancy
- Smoking during pregnancy
- Having gestational diabetes
- Having a low maternal body mass index (BMI)
- Having an early amniocentesis
Women may be able to decrease their chances of having a short umbilical cord by avoiding smoking and drinking alcohol during pregnancy and managing their blood sugar and body weight.
How do I know if my baby is tangled in the umbilical cord?
There are certain signs that a baby might be tangled in an umbilical cord. They include the following:
- Less fetal movement. In the third trimester, there should be a good amount of fetal movement. On average, babies should kick around 5 times in 30 minutes. If a baby is suddenly less active by the 37th week of pregnancy or later, it can indicate that the umbilical cord is wrapped around its neck.
- Forceful movements followed by less movement. If a baby is tangled in the umbilical cord, they often exhibit forceful movements followed by less movement. This happens when the fetus tries to reposition itself to alleviate the pressure around its neck.
- Slower heart rate during labor. If the fetal heart monitor shows that the baby’s heart rate is slowing down considerably, it might be due to a nuchal cord.
Can I do anything to prevent the umbilical cord from getting wrapped around my baby’s neck in the womb?
While you can’t really do anything during pregnancy to prevent a nuchal cord, you may increase your chances of developing umbilical cord problems during delivery by doing the following:
- Avoid being induced.
- Avoid receiving an epidural.
- Avoid having your membranes ruptured.
- Move around and avoid staying in bed for long stretches leading up to delivery.
How can umbilical cord injuries be prevented?
Umbilical cord injuries can be prevented when doctors recognize a potential problem early. A cesarean section is one of the solutions as it can help avoid membranes from rupturing. Additionally, if a doctor realizes that there’s a problem with the umbilical cord during delivery, they should take immediate measures to prevent the baby from potentially suffering from asphyxia.
Can the umbilical cord strangle my baby?
There is a long-standing myth that if the umbilical cord is wrapped around a baby’s neck, it commonly leads to strangulation in the womb. This is not true. The umbilical cord is made to handle temporary squeezing and compression and is also cushioned by a protective layer of Wharton’s jelly, so it poses little risk to a baby’s health when wrapped around the neck in the womb.
Babies very rarely die during pregnancy from umbilical cord strangulation. The bigger risk happens during delivery, but even that can be easily managed by competent medical professionals.
What should doctors do during delivery if the cord is wrapped around my baby’s neck?
If the doctor sees that the umbilical cord is around the baby’s neck during delivery, they can assess the situation to determine the best course of action. If it’s loose enough, the cord can often be slipped over the baby’s head before its body is delivered. In these situations, the mother will be instructed not to push until the cord is loosened.
Sometimes, the cord is too tight and needs to be cut prior to delivery. This hastens the birth because it means the baby can no longer get essential nutrients through the umbilical cord. In some cases, a C-section is necessary to prevent complications.
Contact a cerebral palsy and birth injury attorney
Getting help for a child with a birth injury can make a big difference. Early intervention and treatment are often key to helping improve a child’s well-being, so the sooner you act, the better.
If you have questions about whether your child’s birth injury was caused by a preventable medical error, birth injury attorney Laura Brown at Brown Trial Firm may be able to help. Laura has years of experience in birth injury law, helping families like yours all across the U.S. get the compensation they deserve. She can also point you to great non-legal resources that can help you figure out your next steps.
Contact her today for a free consultation of your case.
- Cerebral Palsy
- Caput Succedaneum and Cephalohematoma
- Neonatal Intracranial Hemorrhage (Childbirth Brain Bleeds)
- Hydrocephalus (Extra Fluid in the Brain Cavity)
- Cervical Dystonia
- Hemiplegia (Brain or Spinal Cord Injury)
- Hemorrhagic Stroke
- Neonatal Stroke
- HIE
- Periventricular Leukomalacia (PVL) Brain Injury
- Infant Seizures
- Spastic Diplegia (Spasticity in the Legs)
- Top Risks for Birth Injuries
- Fetal Alcohol Syndrome
- Facial Paralysis
- Spinal Cord Injuries
- Bell’s Palsy
- Brachial Plexus Nerves & Erb’s Palsy
- Klumpke’s Palsy
- G-Tubes for Newborns
- Medical Errors
- Cesarean Section & Birth Injury
- Negligence in Brain Cooling Treatment
- Craniosacral Therapy
- Occupational Therapy
- Speech Therapy
- Transition From Pediatric to Adult Healthcare
- Surgical Options for Spastic Cerebral Palsy
- Fetal Intolerance to Labor
- Jaundice (Kernicterus)
- Breech Position
- Placental Complications
- Placental Problems
- Umbilical Cord Problems
- Uterine Rupture
- Cervical Incompetence (Insufficiency)
- Blighted Ovum
- Necrotizing Enterocolitis (NEC) - Intestinal Inflammation
- Cephalopelvic Disproportion
- Meconium Aspiration Syndrome
- Amniotic Fluid Embolism
- Birth Injury from Premature Delivery
- Developmental Delays
- Abnormal Cord Insertion
- Infections at Birth
- Chorioamnionitis Bacterial Infection
- Premature birth
- Oxygen Deprivation
- Listeria
- Birth-Acquired Herpes
- Placenta Previa
- Placental Abruption
- Mismanaged Fetal Malposition
- Rapid Labor
- Obesity Related Birth Injuries
- Intrauterine Growth Restriction
- Blood Clots During Pregnancy
- Ectopic Pregnancy Misdiagnosis
- Myths & Facts About Birth Injuries
- Bacterial Vaginosis
- Gestational Diabetes
- Maternal Mortality Risk
- Oligohydramnios (Low Amniotic Fluid)
- Infections During Pregnancy
- Excessive Bleeding During Pregnancy
- Congenital Syphilis


