When a woman experiences uterine rupture during labor or delivery, it could kill or seriously injure the baby and the mother. If you or a loved one has suffered this type of serious injury during labor, it may be in your best interest to get more information about your legal rights and options. You may have a potential medical malpractice claim if the doctor or healthcare provider:
- Used powerful drugs such as Cytotec or Cervidil for off-label purposes
- Gave Cytotec to a mother in labor who had a C-section before (VBAC)
- Failed to provide continuous fetal monitoring
- Failed to recognize the early signs of uterine rupture
Hospitals and medical providers who have caused harm to patients through an act of malpractice can be held accountable for damages that the patient and the baby suffer as a result, including medical bills, future medical and rehabilitation costs, lost wages, pain and suffering, and other related damages.
Signs of uterine rupture include:
Abnormal fetal heart rate. The baby’s heart rate may slow, sometimes dramatically, indicating fetal distress and lack of blood flow and oxygen to the baby.
- Weakening contractions. The strength of the uterine contractions recorded on the fetal heart monitor may weaken, indicating that the muscular uterus is not functioning properly.
- Abdominal pain. The mother may experience a sudden onset of abdominal pain.
- Vaginal bleeding.
- Uterine Rupture and Placental Abruption. When the uterus ruptures, the placenta, which is attached to the wall of the uterus, can also be damaged and may tear away. If the placenta tears away from the wall of the uterus, there may also be a placental abruption. Signs of placental abruption include changes in the baby’s heart rate (fetal heart rate changes or fetal distress), abdominal pain, and vaginal bleeding.
Can Uterine Rupture Cause Birth Asphyxia, Hypoxic-Ischemic Encephalopathy (HIE), and Cerebral Palsy?
Uterine rupture can cause birth asphyxia, hypoxic-ischemic encephalopathy and cerebral palsy. Uterine rupture disrupts the flow of blood to the baby. The blood contains the oxygen that is necessary for the baby’s brain and other vital organs. When uterine rupture deprives the baby of blood and oxygen, the baby develops asphyxia. The asphyxia damages the brain cells and tissues and results in hypoxic-ischemic encephalopathy which is a brain injury cause by lack of blood and oxygen. That brain injury affects the parts of the baby’s brain that control movement, posture, cognition or thinking. As the child grows, the brain injury that happened because of the uterine rupture manifests with abnormal movements which are diagnosed as cerebral palsy.
Uterine Rupture, Hypoxic-Ischemic Encephalopathy (HIE) and Cerebral Palsy Cases
Our birth injury attorneys have experience with uterine rupture cases. We represented a young boy whose mother suffered a uterine rupture. The umbilical cord protruded through the rupture and was compressed causing the boy to suffer asphyxia, hypoxic-ischemic encephalopathy and cerebral palsy.
If you had a uterine rupture and your child suffered an injury, you should determine whether the uterine rupture and your child’s injury could have been prevented. We will investigate the events leading up to the uterine rupture and determine whether proper medical care should have prevented the injury. We will be glad to talk to you about these issues and give you advice about your legal rights and the rights of your child.
 Picture of a normal, fully intact, healthy uterus and lining
Picture of a normal, fully intact, healthy uterus and lining
What is Uterine Rupture?
Uterine rupture is a dangerous complication of pregnancy that can be life-threatening to the mother and the baby. The uterus is the organ in the mother’s body that holds the baby during pregnancy. The uterus is also referred to as the mother’s “womb.” The uterus is a muscular organ that contracts during labor to force the baby through the birth canal for a vaginal delivery.
The placenta is an organ that the mother’s body creates during pregnancy to nourish the baby. The placenta attaches to the inside of the mother’s uterus and then connects to the baby through the umbilical cord. The mother provides oxygen and nutrients to the baby through the placenta and the umbilical cord.
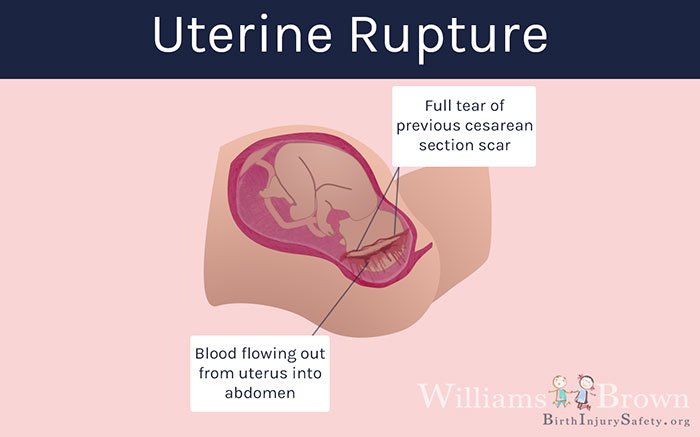
Uterine rupture is a tear or rupture of the uterine wall through some or all of the uterine tissue layers. Uterine rupture is associated with bleeding which can be severe. It can also put the baby in danger by causing fetal distress and abnormal fetal heart rate patterns which are signs that the baby is not getting enough oxygen because of the rupture.
Uterine rupture can also cause that baby to be extruded or forced out of the mother’s uterus into the mother’s abdominal cavity. If the uterus tears or ruptures, the baby can be deprived of blood flow from the mother (ischemia) or deprived of oxygen (hypoxia), which can lead to birth asphyxia, hypoxic-ischemic encephalopathy (HIE) and, later, cerebral palsy. Uterine rupture is a medical emergency and may require an immediate Cesarean section delivery to protect the baby and the mother.
Delays in cesarean section (c-section) delivery when there has been a uterine rupture can result in serious injury or death.
Signs of Uterine Rupture
- Fetal heart rate changes or abnormalities: Bradycardia (heart rate that is too low) is the most common sign of uterine rupture. When the uterus ruptures, the flow of blood and oxygen to the baby is slowed or stopped. The baby’s heart rate responds to the drop in blood flow and oxygen by slowing down to a dangerously low rate.
- Abdominal pain: Abdominal or stomach area pain is a common sign of uterine rupture. The location, severity and character of the abdominal pain may vary. A sudden and severe onset of abdominal pain is an important warning sign of uterine rupture.
- Bleeding: When the uterus ruptures, there is usually bleeding in the abdomen which may bleed out of the vagina. Bleeding may or may not be heavy from the vagina.
- Maternal Hypotension: mother’s blood pressure drops.
- Maternal tachycardia: Mother’s heart rate increases to a high rate.
- Loss of station: The station of the baby refers to the location of the baby in the birth canal. If the baby is extruded or forced out of the uterus through the rupture, the baby’s station in the birth canal may change as all or part of the baby is forced into the abdomen.
- Uterine tenderness: Rupture may be accompanied by uterine tenderness.
- Loss of contractions: Because the muscular uterine wall has been disrupted and all or part of the baby may have been forced out, sometimes the uterine contractions cease.
Risk Factors for Uterine Rupture
VBAC Delivery (Vaginal Birth After Cesarean)
Vaginal birth after Cesarean (VBAC) is when a baby is delivered vaginally after the mother has previously delivered a baby by Cesarean section. Uterine rupture is a known risk in a VBAC delivery. VBAC refers to “vaginal birth after Cesarean” delivery.
A mother who has previously had a Cesarean section has a scar on her uterus from the incision. A scarred uterus is weaker and, therefore, there is a risk that the scarred uterus could tear open during labor allowing the baby, the placenta, or the umbilical cord to stick out or poke through the uterus into the abdominal cavity.
 Picture of an incision scar from previous Cesarean section
Picture of an incision scar from previous Cesarean section
The umbilical cord can be compressed which disrupts the flow of blood and oxygen to the baby. If the placenta is damaged and/or the uterus is damage, those physical injuries can also disrupt the flow of blood and oxygen. This is a type of birth trauma that can result in lack of blood flow and lack of oxygen to the baby causing birth asphyxia, brain injury caused by lack of oxygen (hypoxic-ischemic encephalopathy) and ultimately cerebral palsy.
Hospitals, doctors, and nurses must be aware of the dangers that a VBAC delivery poses to the mother and her child, including the potential for uterine rupture and injury to the baby.
Uterine Rupture and Cesarean (C-section) Delivery
When the mother’s uterus ruptures, an urgent or emergent cesarean (c-section) delivery may be necessary. The uterine rupture can cause significant blood loss which can put the lives of both the mother and the baby at risk. Surgery may be necessary to stop the bleeding and to deliver the baby so the baby can be oxygenated outside of the mother. Delays in recognizing a uterine rupture and delays in performing a cesarean section delivery can cause injury or death to the mother or the baby.
 Picture of uterine rupture and c-section
Picture of uterine rupture and c-section
- Cerebral Palsy
- Caput Succedaneum and Cephalohematoma
- Neonatal Intracranial Hemorrhage (Childbirth Brain Bleeds)
- Hydrocephalus (Extra Fluid in the Brain Cavity)
- Cervical Dystonia
- Hemiplegia (Brain or Spinal Cord Injury)
- Hemorrhagic Stroke
- Neonatal Stroke
- HIE
- Periventricular Leukomalacia (PVL) Brain Injury
- Infant Seizures
- Spastic Diplegia (Spasticity in the Legs)
- Top Risks for Birth Injuries
- Fetal Alcohol Syndrome
- Facial Paralysis
- Spinal Cord Injuries
- Bell’s Palsy
- Brachial Plexus Nerves & Erb’s Palsy
- Klumpke’s Palsy
- G-Tubes for Newborns
- Medical Errors
- Cesarean Section & Birth Injury
- Negligence in Brain Cooling Treatment
- Craniosacral Therapy
- Occupational Therapy
- Speech Therapy
- Transition From Pediatric to Adult Healthcare
- Surgical Options for Spastic Cerebral Palsy
- Fetal Intolerance to Labor
- Jaundice (Kernicterus)
- Breech Position
- Placental Complications
- Umbilical Cord Problems
- Uterine Rupture
- Cervical Incompetence (Insufficiency)
- Blighted Ovum
- Necrotizing Enterocolitis (NEC) - Intestinal Inflammation
- Cephalopelvic Disproportion
- Meconium Aspiration Syndrome
- Amniotic Fluid Embolism
- Birth Injury from Premature Delivery
- Developmental Delays
- Abnormal Cord Insertion
- Infections at Birth
- Chorioamnionitis Bacterial Infection
- Premature birth
- Oxygen Deprivation
- Listeria
- Birth-Acquired Herpes
- Placenta Previa
- Placental Abruption
- Mismanaged Fetal Malposition
- Rapid Labor
- Obesity Related Birth Injuries
- Intrauterine Growth Restriction
- Blood Clots During Pregnancy
- Ectopic Pregnancy Misdiagnosis
- Myths & Facts About Birth Injuries
- Bacterial Vaginosis
- Gestational Diabetes
- Maternal Mortality Risk
- Oligohydramnios (Low Amniotic Fluid)
- Infections During Pregnancy
- Excessive Bleeding During Pregnancy
- Congenital Syphilis


